Tennis Elbow Treatment in Malaysia: From Pain Relief to Full Recovery
Suffering from elbow pain in Malaysia? Discover the full range of treatment options — from physiotherapy and ESWT to PRP injections and surgery — and learn why physio is the clinically preferred first-line intervention.
Book Clinical Assessment Now
What Is Tennis Elbow and Why Is It So Common in Malaysia?
Tennis elbow — clinically termed lateral epicondylitis — is a painful overuse condition affecting the tendons that attach the forearm extensor muscles to the bony prominence on the outer elbow (the lateral epicondyle). Despite its name, the condition is not limited to athletes: the vast majority of cases in Malaysia occur in office workers, construction labourers, factory floor workers, and homemakers performing repetitive wrist and forearm motions.
In Malaysia's working population, the condition is widely underreported because many patients self-medicate with over-the-counter NSAIDs (non-steroidal anti-inflammatory drugs) or topical analgesic creams — managing the pain temporarily without addressing the underlying tendinopathic degeneration at the tissue level.
At the cellular level, the pathology is more accurately described as tendinosis rather than classic inflammation: the extensor carpi radialis brevis (ECRB) tendon undergoes angiofibroblastic degeneration, with disorganised collagen fibres, neovascularisation, and the absence of inflammatory cells. This distinction is clinically significant because it explains why anti-inflammatory drugs alone provide only short-term relief.
Who Gets Tennis Elbow in Malaysia?
The condition disproportionately affects:
Office WorkersKL, Petaling Jaya & Cyberjaya — 8–10 hours daily on keyboard and mouse use
Manual WorkersConstruction, automotive & manufacturing across Selangor and Johor Bahru
HomemakersRepetitive wringing, scrubbing, and lifting tasks
Badminton & Squash PlayersRacket sports with extremely high participation rates in Malaysia
MusiciansParticularly guitarists and pianists in urban centres like Georgetown, Penang
Peak onset typically occurs between ages 35 and 55, though younger patients in manual occupations present increasingly early.
How Is Tennis Elbow Diagnosed in Malaysia?
Tennis elbow is primarily a clinical diagnosis — no imaging is required in straightforward presentations. A qualified clinician or physiotherapist will assess the condition using a structured physical examination.
Key Diagnostic Tests
| Test | What It Assesses | Positive Finding |
|---|---|---|
| Cozen’s Test | ECRB tendon integrity under load | Pain at lateral epicondyle on resisted wrist extension |
| Mill’s Test | Passive stretch of extensor mechanism | Pain with elbow extended, forearm pronated, wrist flexed |
| Maudsley’s Test | Extensor digitorum involvement | Pain on resisted middle finger extension |
| Grip Strength Assessment | Functional deficit quantification | Reduced grip vs. contralateral side |
When the diagnosis is uncertain or conservative treatment has failed after 6 weeks, clinicians in Malaysian hospitals and sports medicine centres may order:
Diagnostic Ultrasound (US)
First-line imaging; visualises tendon thickening, calcification, hypoechoic zones, and neovascularisation in real time. Available at most KPJ, Pantai, and Sunway Medical centres.
MRI
Reserved for complex or surgical cases; superior soft tissue resolution to rule out ligament involvement or occult fracture.
X-Ray
Ordered primarily to exclude bony pathology such as loose bodies or calcific deposits within the joint.
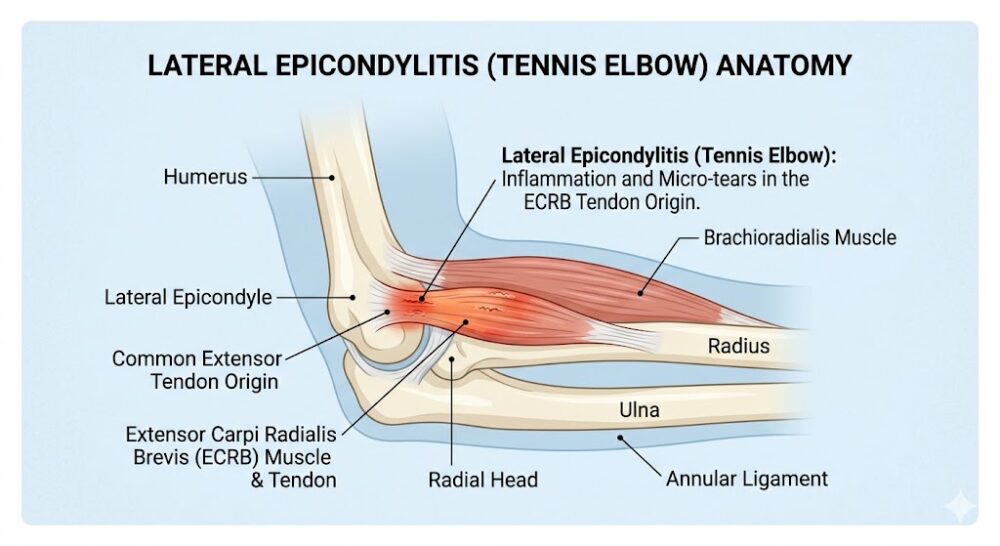 Annotated anatomy of the lateral elbow showing the lateral epicondyle, ECRB tendon insertion point, and area of degeneration in tennis elbow.
Annotated anatomy of the lateral elbow showing the lateral epicondyle, ECRB tendon insertion point, and area of degeneration in tennis elbow.What Are the Treatment Options for Tennis Elbow in Malaysia?
Tennis elbow treatment in Malaysia follows a staged, evidence-based protocol — beginning with conservative management and escalating to invasive interventions only when first-line approaches have been exhausted.
These are the universally recommended first-line interventions and account for the successful resolution of 80–95% of tennis elbow cases without any procedural intervention.
Activity Modification and Load Management
The first and most critical step is reducing or temporarily eliminating the repetitive mechanical loading that perpetuates the tendinopathy. This does not mean complete rest — prolonged immobilisation is counterproductive to tendon remodelling. Instead, a graded relative rest strategy is applied:
- Identify and avoid specific provocative movements (repetitive wrist extension under load)
- Ergonomic workstation review for keyboard users in Klang Valley office environments
- Technique correction for racket sports players (grip size, string tension, stroke mechanics)
Physiotherapy (The Clinical Gold Standard)
Physiotherapy is the single most evidence-supported treatment modality for tennis elbow, consistently endorsed by systematic reviews and clinical guidelines from bodies including the British Journal of Sports Medicine and the American College of Physicians. The Malaysian Physiotherapy Association (MPA) similarly positions physiotherapy as the preferred first-line intervention over corticosteroid injection for lateral epicondylitis.
A structured physiotherapy programme for tennis elbow in Malaysia typically includes:
- Eccentric and isometric strengthening exercises: The cornerstone of tendon rehabilitation. Eccentric loading — lengthening the muscle under tension — drives collagen remodelling and restores tensile strength to the degenerated ECRB tendon. Isometric holds are increasingly used in the acute phase for immediate analgesic effect.
- Manual therapy: Joint mobilisation techniques targeting the radial head and inferior radioulnar joint have been shown to produce immediate hypoalgesic effects and improve grip strength. Soft tissue release to the forearm extensor muscle belly reduces centralised neuromotor facilitation.
- Dry needling: Intramuscular stimulation of myofascial trigger points in the extensor carpi radialis muscles desensitises the peripheral nociceptive system and promotes local blood flow to the tendon insertion.
- Taping and bracing: Kinesiology taping (KT tape) applied to the forearm extensor compartment offloads compressive forces at the lateral epicondyle. A counterforce brace (tennis elbow strap) reduces peak strain at the tendon insertion during activity.
- Patient education and self-management: Physiotherapists provide guided home exercise programmes, activity pacing strategies, and ergonomic advice — essential for the large proportion of patients in sedentary desk jobs across Kuala Lumpur and its satellite cities.
Typical duration: 6–12 weeks of structured physiotherapy, with measurable pain and functional improvements expected within 4–6 weeks for most patients.
Topical and Oral NSAIDs
Topical NSAIDs such as diclofenac gel (Voltaren) or ibuprofen cream are recommended over oral NSAIDs for tennis elbow due to their comparable local efficacy with substantially lower systemic side effect profiles. Oral NSAIDs (e.g., naproxen, celecoxib) may be used short-term for acute flare management but are not appropriate as a standalone long-term strategy given the non-inflammatory nature of the underlying tendinopathy.
Important: In Malaysia, NSAIDs require a prescription from a registered medical practitioner under Akta Dadah Berbahaya 1952 amendments for certain formulations. Patients with a history of peptic ulcer disease, chronic kidney disease, or cardiovascular conditions should consult their physician before initiating oral NSAID therapy.
Counterforce Bracing
An elbow counterforce brace (lateral epicondylitis strap) applies compressive pressure to the proximal forearm muscle belly, effectively reducing the tensile force transmitted to the inflamed tendon insertion. These are widely available at Watson’s, Guardian, and physiotherapy clinics throughout Malaysia for RM 25–RM 80. They are most effective when used in conjunction with physiotherapy, not as a standalone intervention.
When 6–12 weeks of structured conservative management has failed to achieve adequate pain relief and functional restoration, the following procedural options are available through Malaysian sports medicine physicians, orthopaedic specialists, and musculoskeletal radiologists.
Corticosteroid Injection (CSI)
Corticosteroid injections (typically triamcinolone acetonide or methylprednisolone combined with lidocaine) are among the most commonly offered short-term interventions for tennis elbow in Malaysian private medical centres and specialist clinics.
What the evidence says: CSI produces superior short-term pain relief at 4–6 weeks compared to physiotherapy, but long-term outcomes (at 12 months and beyond) are significantly worse — with higher recurrence rates and poorer tendon integrity than physiotherapy-treated patients. A landmark 2013 trial published in The Lancet demonstrated that patients who received CSI had worse 1-year outcomes than the wait-and-see group.
Current clinical position in Malaysia: Leading orthopaedic and sports medicine specialists at institutions such as Hospital Kuala Lumpur (HKL), National Sports Institute (ISN), and private centres (Beacon, Gleneagles) now recommend limiting corticosteroid injections to no more than 2–3 lifetime injections at a single site, due to risks of tendon atrophy, rupture, subcutaneous fat necrosis, and skin depigmentation (a particularly noted concern among Malaysian patients with Fitzpatrick skin types III–V).
Platelet-Rich Plasma (PRP) Injection
PRP therapy involves the centrifugation of the patient’s own blood to concentrate platelets — rich in growth factors including PDGF, TGF-β, and VEGF — which are then injected directly into the degenerative tendon under ultrasound guidance to stimulate collagen synthesis and tissue regeneration.
PRP is increasingly available at sports medicine and orthopaedic centres in Kuala Lumpur, Petaling Jaya, and Penang. Evidence supports PRP as superior to CSI at 6 and 12 months, with the advantage of promoting genuine tissue healing rather than suppressing the inflammatory cascade.
Extracorporeal Shock Wave Therapy (ESWT)
ESWT delivers high-energy acoustic pressure waves to the tendon insertion, triggering a neovascularisation response and disrupting pathological nerve fibres that mediate chronic tendon pain. It is a non-invasive, office-based procedure requiring no anaesthesia.
Available at selected physiotherapy centres and sports medicine clinics in Klang Valley, Johor Bahru, and Penang, ESWT has demonstrated efficacy particularly in chronic cases (>3 months duration) and calcific presentations. A typical course involves 3–5 sessions at weekly intervals.
Prolotherapy
Prolotherapy involves injection of a hypertonic dextrose solution into the lateral epicondyle and surrounding ligamentous structures to provoke a controlled inflammatory response and stimulate connective tissue repair. It is less widely offered in Malaysia than PRP but available at select integrative medicine and pain management clinics. Evidence is emerging but remains less robust than for PRP.
Surgery is reserved for a small minority of patients (estimated at 5–10%) who fail a minimum of 6 months of rigorous conservative management including physiotherapy and at least one procedural intervention.
Surgical Release (Open or Arthroscopic)
The standard surgical procedure is débridement and release of the degenerated ECRB tendon from the lateral epicondyle. This can be performed via:
- Open technique: A 2–4 cm incision over the lateral epicondyle, direct visualisation and excision of pathological tissue, followed by tendon reattachment or repair.
- Arthroscopic technique: Minimally invasive approach through 2–3 portal incisions; associated with faster return to activity and lower risk of post-operative stiffness.
Both procedures are performed under general or regional anaesthesia at accredited Malaysian private hospitals (KPJ, Pantai, Sunway, Gleneagles) and public specialist hospitals. Post-operative physiotherapy rehabilitation is mandatory for 8–12 weeks to restore full strength and range of motion.
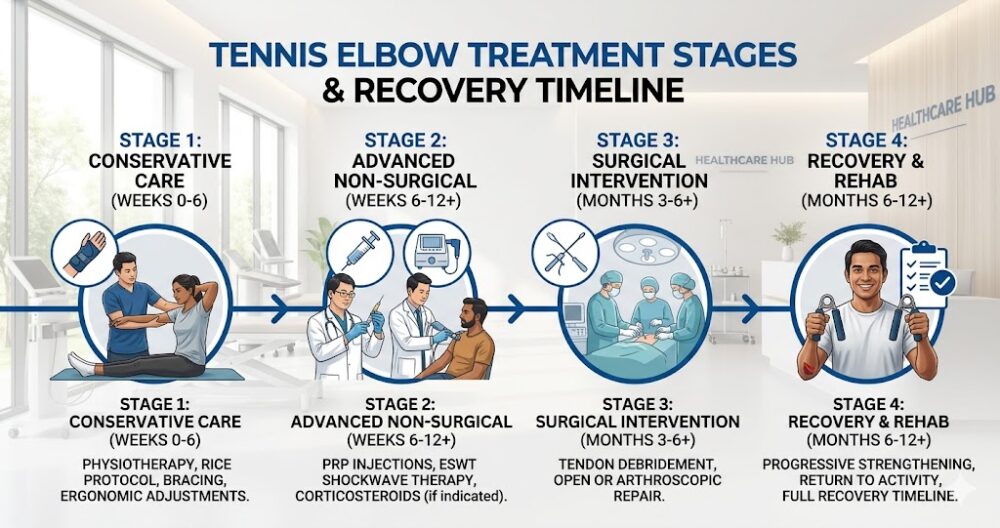 Tennis elbow treatment timeline: from physiotherapy through to surgery, with expected recovery durations at each stage.
Tennis elbow treatment timeline: from physiotherapy through to surgery, with expected recovery durations at each stage.Why Physiotherapy Is the Recommended First-Line Treatment for Tennis Elbow
Physiotherapy is the most recommended first-line treatment for tennis elbow because it is the only modality that directly addresses the underlying mechanism of the condition — tendon remodelling through progressive mechanical loading — rather than masking symptoms.
The evidence base supporting physiotherapy for lateral epicondylitis is extensive:
- Systematic reviews consistently demonstrate equivalent or superior long-term outcomes for physiotherapy compared to corticosteroid injection (the most common alternative in Malaysian clinical practice).
- Eccentric exercise protocols produce measurable histological changes in the degenerated tendon — increased collagen fibre organisation, reduced neovascularisation, and normalised tenocyte morphology — that pharmacological or injection therapies do not replicate.
- Recurrence rates following physiotherapy-led rehabilitation (estimated at 8–12% at 2 years) are substantially lower than those following corticosteroid injection alone (estimated at 30–70% at 1 year in multiple controlled trials).
- Malaysian Ministry of Health (MOH) Clinical Practice Guidelines for musculoskeletal conditions endorse graded exercise-based rehabilitation as the cornerstone of tendinopathy management.
What to Expect at a Tennis Elbow Physiotherapy Assessment in Malaysia
A comprehensive initial physiotherapy assessment for tennis elbow typically takes 45–60 minutes and includes:
- Subjective history: Onset, mechanism, occupation, sport participation, prior treatments
- Objective examination: Cozen’s, Mill’s, and Maudsley’s tests; grip dynamometry; cervical spine screen (to exclude referred pain from C5–C6 nerve root)
- Functional assessment: Provocative tasks relevant to the patient’s occupation or sport
- Treatment planning: Individualised programme with short- and long-term goal-setting
- First treatment session: Often commences within the same appointment — manual therapy, taping, and initial exercise instruction
The physiotherapist will also advise on realistic recovery timelines based on symptom duration and severity — a critical piece of information that helps Malaysian patients make informed decisions about whether to continue conservative management or pursue procedural options.
Tennis Elbow Treatment Cost Comparison in Malaysia
| Treatment Modality | Approximate Cost (RM) | Session Frequency | Invasiveness | Best For |
|---|---|---|---|---|
| Physiotherapy | RM 60–RM 150/session | 1–2× per week, 6–12 weeks | Non-invasive | All stages; first-line |
| Counterforce Brace | RM 25–RM 80 | One-time | Non-invasive | Adjunct to physio |
| ESWT | RM 200–RM 500/session | 3–5 sessions | Non-invasive | Chronic/calcific cases |
| Corticosteroid Injection | RM 200–RM 500/episode | Max 2–3 lifetime | Minimally invasive | Short-term relief only |
| PRP Injection | RM 500–RM 1,500/session | 1–3 sessions | Minimally invasive | Moderate-to-severe, chronic |
| Prolotherapy | RM 300–RM 800/session | 3–6 sessions | Minimally invasive | Ligamentous laxity component |
| Surgery (open/arthroscopic) | RM 8,000–RM 25,000 | One procedure | Surgical | Refractory cases only |
Costs are indicative ranges for Klang Valley private practice (2024–2025). Public hospital (KKM) rates are substantially lower but subject to waiting time constraints.
How Long Does Tennis Elbow Take to Heal With Physiotherapy in Malaysia?
Recovery time depends primarily on symptom duration at the point of treatment initiation — the single most important prognostic factor:
| Symptom Duration at First Treatment | Expected Recovery With Physiotherapy |
|---|---|
| < 3 months (acute) | 6–8 weeks |
| 3–6 months (subacute) | 8–16 weeks |
| > 6 months (chronic) | 16–24+ weeks; procedural adjuncts may be indicated |
| Post-surgical rehabilitation | 8–12 weeks post-op before return to full activity |
The clinical takeaway is unambiguous: earlier physiotherapy intervention produces faster and more complete recovery. Patients who delay treatment — often due to self-medicating with over-the-counter pain relief — accumulate greater tendon pathology and face proportionally longer rehabilitation journeys.
Frequently Asked Questions About Tennis Elbow Treatment in Malaysia
Mild cases of tennis elbow can self-resolve over 12–18 months with activity modification alone, but untreated cases frequently become chronic and recurrent. Seeking early physiotherapy significantly reduces total recovery time and prevents the condition from progressing to severe tendinopathy requiring injections or surgery.
Most Malaysian private medical insurance (from providers such as AIA, Great Eastern, Prudential, and Allianz) covers physiotherapy for lateral epicondylitis when referred by a registered medical practitioner (RM) and performed at an accredited clinic. Patients should verify their plan’s annual physiotherapy benefit limit, as most standard policies cap coverage at RM 3,000–RM 5,000 per year. Government employees under SOCSO (PERKESO) may be eligible for physiotherapy coverage under the Employment Injury Scheme if the condition is work-related.
Tennis elbow (lateral epicondylitis) affects the outer elbow at the lateral epicondyle — the extensor tendons on the dorsal forearm. Golfer’s elbow (medial epicondylitis) affects the inner elbow at the medial epicondyle — the flexor-pronator tendons on the volar forearm. Both are overuse tendinopathies, but their pain location, provocative movements, and management protocols differ. A physiotherapy assessment can accurately differentiate between the two conditions and rule out other causes of elbow pain such as radial tunnel syndrome or posterior interosseous nerve entrapment.
For a new presentation of tennis elbow without neurological symptoms (numbness, tingling, or weakness radiating into the hand), a physiotherapist should be your first point of contact. Physiotherapists are trained to diagnose lateral epicondylitis, design a complete rehabilitation programme, and determine when onward referral is warranted. Bypassing physiotherapy and proceeding directly to a surgeon often leads to unnecessary procedural interventions. However, if you are also experiencing persistent tingling into the fingers, a physiotherapist can accurately differentiate between tendinopathy and conditions requiring non-surgical relief for carpal tunnel syndrome or hand numbness in the Klang Valley.
Most patients with acute-to-subacute tennis elbow require between 8 and 16 sessions of physiotherapy spread over 6–12 weeks. Chronic cases may require 20–24 sessions. Your physiotherapist will reassess your progress at regular intervals (typically every 4–6 sessions) and adjust the programme accordingly. Compliance with home exercises prescribed between sessions is a critical determinant of outcome.
ESWT and PRP are adjunctive or escalation therapies — they are indicated when physiotherapy alone has not achieved adequate results after 6–12 weeks, not as replacements. When combined with physiotherapy, both ESWT and PRP demonstrate improved outcomes over either modality alone. No high-quality evidence supports using ESWT or PRP as a first-line intervention ahead of a structured physiotherapy programme.
During the acute phase (first 4–6 weeks of treatment), racket sports should be significantly reduced or temporarily paused. As pain subsides and tissue loading capacity improves through physiotherapy, a graded return-to-sport protocol is implemented. Your physiotherapist will guide you through progressive racket sport activity — adjusting grip size (a thicker grip reduces peak extensor tendon strain), string tension, and session duration — before returning to full unrestricted play. Attempting to play through pain delays tissue remodelling and risks progressing the tendinopathy.
Verified physiotherapy and rehabilitation services for tennis elbow are available at our partner centre in Sungai Buloh, conveniently accessible from Kepong, Kota Damansara, Rawang, and the broader northern Klang Valley. You can find comprehensive care and book your appointment at our dedicated rehab centre here.
📅 Book Your Tennis Elbow Assessment in the Klang Valley
Whether you suspect tennis elbow or another elbow condition, the right diagnosis is everything. Our vetted physiotherapy partners across Sungai Buloh and the Klang Valley provide accurate clinical assessment and condition-specific rehabilitation from the very first session. No GP referral required.
Tap your location to open WhatsApp — no forms, no waiting.
The information in this article is intended for general educational purposes and does not constitute medical advice. Always consult a clinician registered with the Malaysian Medical Council (MMC) or a physiotherapist registered with the Malaysian Physiotherapy Association (MPA) for a diagnosis and personalised treatment plan. ServicePro.my connects Malaysians with vetted, verified healthcare and home service professionals across the Klang Valley and beyond.



