How to Treat Shoulder Impingement Without Surgery in the Klang Valley
Up to 80% of shoulder impingement cases resolve successfully with structured, non-surgical treatment — provided it is started early and administered correctly. This guide gives you a clinically grounded, Malaysia-specific roadmap to full recovery.
Book Clinical Assessment Now
What Exactly Is Shoulder Impingement Syndrome?
Shoulder impingement occurs when the rotator cuff tendons or the subacromial bursa become mechanically compressed between the head of the humerus and the acromion bone during arm elevation. This compression triggers inflammation, pain, and progressive functional loss if left untreated.
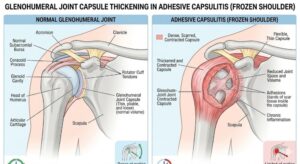
Because symptoms often overlap with adhesive capsulitis, knowing how to tell if it's frozen shoulder or impingement is a critical first step before attempting any self-rehabilitation.
It is classified into two primary categories:
Caused by structural factors such as an abnormally shaped (hooked or curved) acromion, reducing the subacromial space from birth or over time.
Far more common in active adults and office workers. Caused by muscular imbalances, poor posture, and rotator cuff weakness — all of which allow the humeral head to migrate upward into the acromion during movement.
Why Is Shoulder Impingement Increasingly Common in Klang Valley?
Several Malaysia-specific lifestyle factors are driving a rise in shoulder impingement presentations at physiotherapy clinics across Petaling Jaya, Shah Alam, Subang Jaya, and Kuala Lumpur:
Prolonged Desk-Bound Postures
IT, finance, and civil service workers in the Klang Valley frequently develop the rounded-shoulder, forward-head posture that is the single greatest modifiable risk factor for secondary impingement.
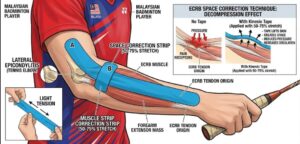
Badminton Culture
Malaysia is one of the world’s most badminton-obsessed nations. The repetitive overhead smash motion is a primary mechanical driver of rotator cuff impingement, particularly in recreational players over 35 who do not follow structured warm-up and strengthening protocols.
Gym Injuries
The rise of fitness culture in KL has brought an increase in impingement caused by excessive internal rotation training (bench pressing, front raises) without balancing posterior chain and external rotator work.
Aging Population
Subacromial space naturally narrows with age-related degenerative changes, making Malaysians over 50 significantly more vulnerable.
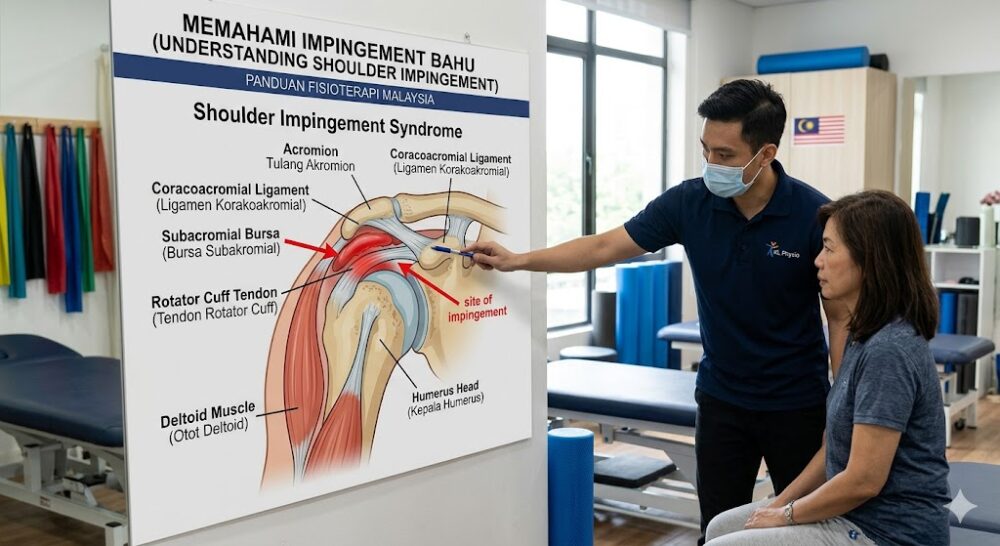 Anatomy of shoulder impingement: the subacromial space and rotator cuff tendons under compression during arm elevation.
Anatomy of shoulder impingement: the subacromial space and rotator cuff tendons under compression during arm elevation.How Is Shoulder Impingement Diagnosed in Malaysia?
Shoulder impingement is diagnosed through a combination of clinical physical examination tests, patient history, and imaging — typically an X-ray and, in more complex cases, an MRI. You do not need to go to a hospital emergency department for this diagnosis; a registered physiotherapist or an orthopaedic specialist at a private clinic in the Klang Valley can conduct the initial assessment.
Key Diagnostic Tests Your Clinician Will Perform
| Test Name | What It Assesses |
|---|---|
| Neer’s Sign | Pinching of the supraspinatus tendon under the anterior acromion during passive arm elevation |
| Hawkins-Kennedy Test | Subacromial bursa compression via internal rotation; highly sensitive for impingement |
| Empty Can Test (Jobe’s Test) | Supraspinatus tendon integrity and strength deficit |
| Painful Arc Test | Characteristic pain between 60°–120° of abduction, classic for impingement |
| Drop Arm Test | Rules out a full-thickness rotator cuff tear requiring surgical referral |
Red flag: If the Drop Arm Test is positive, or if you experience sudden, significant weakness making it impossible to hold your arm at 90° abduction, you should request an urgent MRI and orthopaedic referral. This may indicate a complete rotator cuff tear, which is a distinct condition requiring a different management pathway.
Do You Need an MRI First?
Not necessarily. In Malaysia’s private healthcare system, a standard shoulder MRI costs between RM 700 – RM 1,500 depending on the centre and whether contrast is used. Many patients with classic impingement presentations are appropriately managed by a physiotherapist without imaging. Your clinician will refer you for MRI if:
- Symptoms have not improved after 6–8 weeks of physiotherapy.
- A partial or complete rotator cuff tear is clinically suspected.
- Symptoms are atypical or neurological involvement is possible.
What Are the Evidence-Based Non-Surgical Treatments for Shoulder Impingement?
The gold standard non-surgical treatment for shoulder impingement is a structured physiotherapy programme lasting 6–12 weeks, combining manual therapy, targeted exercise rehabilitation, and activity modification. This approach is supported by Level 1 clinical evidence and is the first-line recommendation from international orthopaedic bodies.
Here is a breakdown of each therapeutic component:
1 Physiotherapy Exercise Rehabilitation (Primary Treatment)
This is the most important component of conservative management. A qualified physiotherapist in Malaysia will prescribe a progressive programme targeting the specific muscular deficits driving your impingement.
Phase 1 — Pain Control and Range of Motion (Weeks 1–3)
- Pendulum exercises (Codman’s exercises) to decompress the joint gently
- Passive and active-assisted range-of-motion work
- Posture correction drills (scapular retraction, thoracic extension)
- Pain neuroscience education to reduce guarding behaviors
Phase 2 — Strengthening (Weeks 4–8)
- Rotator cuff activation: Side-lying external rotation, prone “Y-T-W” exercises targeting the lower trapezius and serratus anterior
- Scapular stabilization: Serratus anterior activation is critical for restoring scapulohumeral rhythm and “opening” the subacromial space during arm elevation
- Isometric to isotonic progression: Begin with pain-free isometrics before advancing to resistance band and dumbbell loading
Phase 3 — Functional and Sport-Specific Rehabilitation (Weeks 8–12)
- Sport-specific or occupation-specific movement retraining
- Plyometric loading for returning to badminton or overhead sports
- Progressive overhead reaching and loading
2 Corticosteroid Injections (Subacromial Injection)
A corticosteroid (cortisone) injection into the subacromial space provides short-term pain relief of 4–8 weeks, and is most effective when used as an adjunct to physiotherapy, not as a standalone treatment. It is not a cure for impingement.
In Malaysia, subacromial injections are administered by orthopaedic surgeons or sports medicine physicians registered with the Malaysian Medical Council (MMC). The procedure is widely available at private hospitals and sports medicine clinics in the Klang Valley including those in Damansara, Bangsar, and Mont Kiara.
- A maximum of 2–3 injections per year is the standard recommendation to prevent tendon weakening
- The injection is most beneficial when pain levels are so high that a patient cannot engage meaningfully in physiotherapy exercises
- Imaging-guided (ultrasound-guided) injections offer greater precision and are preferable where available
3 Shockwave Therapy (ESWT)
Extracorporeal Shockwave Therapy (ESWT) is an evidence-supported adjunct treatment for chronic shoulder impingement and calcific tendinopathy, reducing pain and promoting tissue healing through acoustic pressure waves. It is particularly useful for cases involving calcific deposits within the rotator cuff tendons.
ESWT is available at a growing number of physiotherapy and sports rehabilitation clinics in Petaling Jaya, Kuala Lumpur, and Subang Jaya. A typical course involves 3–6 sessions at RM 150 – RM 350 per session depending on the clinic and machine used.
4 NSAIDs and Analgesics (Medication)
Non-steroidal anti-inflammatory drugs (NSAIDs) such as naproxen or ibuprofen are recommended for short-term pain management (7–14 days) during the acute phase of shoulder impingement. They reduce subacromial bursa inflammation but do not address the underlying mechanical cause.
Malaysian patients should consult a pharmacist or General Practitioner (GP) before commencing NSAID therapy, particularly if they have pre-existing kidney, cardiovascular, or gastrointestinal conditions.
5 Activity Modification and Ergonomic Correction
Immediately reducing or eliminating the provocative activities — especially overhead reaching, heavy lifting, and repetitive shoulder rotation — is essential to allow tissue healing during the rehabilitation window. For desk-bound workers in Klang Valley offices, an ergonomic workstation assessment is a critical, frequently overlooked component.
Practical ergonomic adjustments for Malaysian office workers:
- Raise your monitor to eye level to prevent the forward-head posture that rolls the shoulders inward
- Keep your keyboard and mouse close to the body to reduce shoulder internal rotation
- Set a posture reminder every 45 minutes if you work from home in a KL condo or landed property without a formal workstation
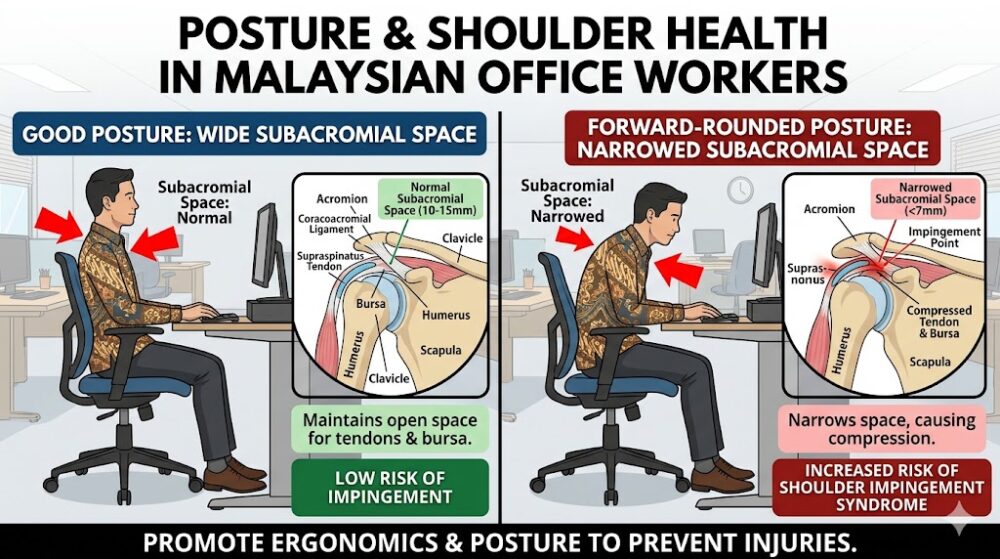 Correct desk posture to prevent and manage shoulder impingement for Malaysian office workers — monitor at eye level, keyboard close to the body.
Correct desk posture to prevent and manage shoulder impingement for Malaysian office workers — monitor at eye level, keyboard close to the body.Best Physiotherapy Exercises for Shoulder Impingement You Can Do at Home
The most effective home exercises for shoulder impingement target the external rotators of the rotator cuff, the lower trapezius, and the serratus anterior — the three muscle groups most consistently weak in impingement patients. Perform these only after receiving a clinical diagnosis. Do not push through sharp or acute pain.
Safety Note: These exercises are for educational reference. They are not a substitute for an individualised assessment by a registered physiotherapist. If you are in Malaysia, look for physiotherapists registered with the Malaysian Physiotherapy Association (MPA).
Home Exercise Programme (Perform Daily, Both Sides)
Scapular Retraction (Postural Reset)
- Sit or stand upright. Gently squeeze your shoulder blades together as if trying to hold a pencil between them.
- Hold for 5 seconds. Release slowly.
- Repeat: 15 repetitions × 3 sets.
Side-Lying External Rotation (Rotator Cuff Activation)
- Lie on your unaffected side. Elbow bent to 90°, upper arm resting against your side.
- Keeping the elbow pinned to the side, slowly rotate the forearm upward toward the ceiling.
- Lower slowly. Use a 0.5–1 kg dumbbell or a water bottle.
- Repeat: 12–15 repetitions × 3 sets.
Prone “T” Exercise (Lower Trapezius)
- Lie face-down on a bed or mat, arms extended to the side at shoulder height (forming a “T” shape), thumbs pointing toward the ceiling.
- Lift both arms slightly off the surface, squeeze shoulder blades. Hold 3 seconds.
- Lower slowly.
- Repeat: 12 repetitions × 3 sets.
Wall Slide with Serratus Activation
- Stand facing a wall, forearms resting on the surface.
- Maintain contact with the wall while pushing your upper back outward (protraction).
- Slowly slide your arms upward while maintaining this protractive pressure. Stop at pain onset.
- Repeat: 10–12 repetitions × 2 sets.
Doorway Pec Stretch (Passive Posterior Capsule Stretch)
- Stand in a doorway with your elbow at 90°, forearm resting on the frame.
- Gently rotate your body away from the arm until you feel a stretch across the chest.
- Hold for 30 seconds.
- Repeat: 3 holds per side.
How Much Does Shoulder Impingement Treatment Cost in Malaysia Without Surgery?
Non-surgical shoulder impingement treatment in Malaysia typically costs between RM 100 – RM 350 per physiotherapy session, with a full rehabilitation programme of 12–20 sessions ranging from RM 1,500 – RM 5,000 in total for private clinic treatment. Costs vary significantly between KL city centre clinics, suburban Petaling Jaya practices, and hospital-based physiotherapy departments.
| Treatment Type | Estimated Cost in Malaysia |
|---|---|
| Private Physiotherapy Session (KL/PJ) | RM 120 – RM 350 per session |
| Government Hospital Physiotherapy (Panel/Referral) | RM 1 – RM 5 per visit (subsidised) |
| Subacromial Cortisone Injection (Private) | RM 350 – RM 800 |
| Shoulder MRI (Private, Without Contrast) | RM 700 – RM 1,200 |
| Shockwave Therapy (ESWT) Per Session | RM 150 – RM 350 |
| Orthopaedic Specialist Consultation (Private) | RM 150 – RM 300 |
Does Malaysian Insurance Cover Physiotherapy?
Many Malaysian medical insurance and Takaful plans cover physiotherapy only when it follows hospitalisation or is referred by a registered medical doctor (RM). Standalone outpatient physiotherapy is frequently excluded from basic plans. Check your policy’s outpatient benefits rider carefully. Companies such as AIA, Prudential, Great Eastern, and Etiqa offer rider upgrades that include outpatient physiotherapy benefits.
When Should Shoulder Impingement Surgery Be Considered in Malaysia?
Surgery for shoulder impingement — typically an arthroscopic subacromial decompression (ASAD) — is only recommended when a structured, consistently applied conservative programme of at least 3–6 months has failed to produce adequate functional improvement. This is the recommendation aligned with both international orthopaedic guidelines and the clinical practice standards observed by specialists under the Malaysian Orthopaedic Association (MOA).
Surgical consideration is appropriate when:
- Pain and dysfunction remain severe after 6 months of rigorous physiotherapy and at least one corticosteroid injection.
- MRI confirms a structural lesion requiring surgical repair (e.g., a full-thickness rotator cuff tear, large calcific deposit, or AC joint pathology).
- The patient’s quality of life and occupational function are severely and measurably impaired.
Critical context for Malaysian patients: Many patients in the Klang Valley are referred to surgery prematurely because they have not completed a full, properly supervised physiotherapy programme. One or two sporadic sessions is not adequate conservative management. Commit to the full structured programme before accepting a surgical referral.
 Conservative physiotherapy versus surgical intervention: outcome comparison for shoulder impingement in the Malaysian context.
Conservative physiotherapy versus surgical intervention: outcome comparison for shoulder impingement in the Malaysian context.Red Flags: Seek Immediate Medical Attention If You Notice
- Sudden severe shoulder pain after a fall or collision — possible rotator cuff tear or fracture
- Shoulder pain accompanied by chest pain, shortness of breath, or left arm radiation — rule out cardiac origin immediately
- Visible deformity, swelling, or bruising after trauma
- Complete inability to hold your arm at 90° abduction (positive Drop Arm Test) — possible full-thickness rotator cuff tear
- Night sweats, unexplained weight loss, or fever alongside shoulder pain — possible systemic or neoplastic cause
📍 Local Note: This guide is written for patients in Sungai Buloh and the Klang Valley corridor. Nearby specialist centres include Hospital Sungai Buloh (HSB), Columbia Asia Hospital Petaling Jaya, Subang Jaya Medical Centre (SJMC), and KPJ Damansara Specialist Hospital. For post-diagnosis physiotherapy, our vetted rehabilitation partners serve patients across Sungai Buloh, Kepong, Shah Alam, Petaling Jaya, and surrounding areas.
Frequently Asked Questions About Treating Shoulder Impingement Without Surgery in Malaysia
Most patients with shoulder impingement see significant improvement within 6–12 weeks of consistent physiotherapy. Full recovery, including return to sport or heavy manual work, typically takes 3–6 months depending on the severity of the condition, the patient’s compliance with the home exercise programme, and how early treatment was initiated.
You should reduce or temporarily stop badminton during the acute and early rehabilitation phases of shoulder impingement treatment. Continuing to play through pain accelerates tendon degeneration and risks partial rotator cuff tears. Your physiotherapist will clear you to return to the court — typically with a modified programme — once the subacromial space has been adequately decompressed through rehabilitation. Most recreational badminton players in Malaysia return to play within 8–16 weeks.
Shoulder impingement is not inherently permanent. Secondary (functional) impingement — the most common type — is highly reversible with correct physiotherapy because it stems from correctable muscular imbalances and postural habits. However, if left unmanaged for years, impingement can lead to partial and eventually full rotator cuff tears, which are far more serious and may require surgery.
For most Klang Valley residents with a new onset of shoulder pain consistent with impingement, a registered physiotherapist is the appropriate first contact. Physiotherapists are trained to screen for serious pathology (red flags) and will refer you to an orthopaedic surgeon or sports medicine physician if clinically indicated. This pathway is faster and more cost-effective than going directly to a specialist and avoids unnecessary imaging costs. Ensure your physiotherapist is registered with the Malaysian Physiotherapy Association (MPA).
Yes. Sleeping on the affected shoulder dramatically increases subacromial compression and is one of the leading reasons patients report worse pain in the morning. Malaysian patients are advised to sleep on their back or on the unaffected side with a pillow supporting the affected arm in a slightly elevated position. Avoid side-sleeping on the painful shoulder entirely until physiotherapy has sufficiently resolved the condition.
Malaysia’s high ambient humidity does not directly worsen shoulder impingement, but sedentary indoor lifestyles driven by heat avoidance contribute to the postural deconditioning that underlies most functional impingement cases. Spending long hours in air-conditioned offices and at home in KL condos in fixed, unsupported postures is a significant contributing factor. Structured movement breaks are essential.
Shoulder impingement refers to the mechanical compression of rotator cuff tendons, while a rotator cuff tear refers to an actual structural breach — partial or complete — in the tendon tissue itself. Impingement, if left untreated, can progress to a rotator cuff tear over time. The distinction matters clinically because complete rotator cuff tears often require surgical repair, whereas impingement without tearing is managed conservatively. An MRI is required to definitively differentiate between the two.
A registered medical doctor (doctor with the MMC), not a physiotherapist, is the only clinician who can issue an MC in Malaysia. If your shoulder impingement is severe enough to prevent safe work performance — particularly for manual workers or those in physically demanding jobs in the Klang Valley’s construction, logistics, or manufacturing sectors — consult a GP or specialist who can document the functional limitation and issue the appropriate medical leave certification.
📅 Book Your Shoulder Impingement Assessment in the Klang Valley
Whether you’re managing a sports injury, desk-related pain, or chronic shoulder stiffness — our vetted physiotherapy partners across Sungai Buloh and the Klang Valley provide accurate clinical assessment and condition-specific rehabilitation from the very first session.
Tap your location to open WhatsApp — no forms, no waiting.
📍 Local Note:
This article is produced by the ServicePro.my Healthcare Editorial Team for informational purposes only. It does not constitute medical advice. Always consult a licensed healthcare professional — including a registered physiotherapist, orthopaedic surgeon, or GP — for diagnosis and individualised treatment planning.