Sakit Bahu? How to Tell If It’s Frozen Shoulder or Shoulder Impingement (And How to Fix It)
Frozen shoulder and shoulder impingement are the two most common causes of persistent sakit bahu in Malaysian adults — but they require completely different treatments. Misidentifying one for the other is why so many Malaysians spend months on painkillers without improvement.
Consult a Verified Sungai Buloh Physiotherapist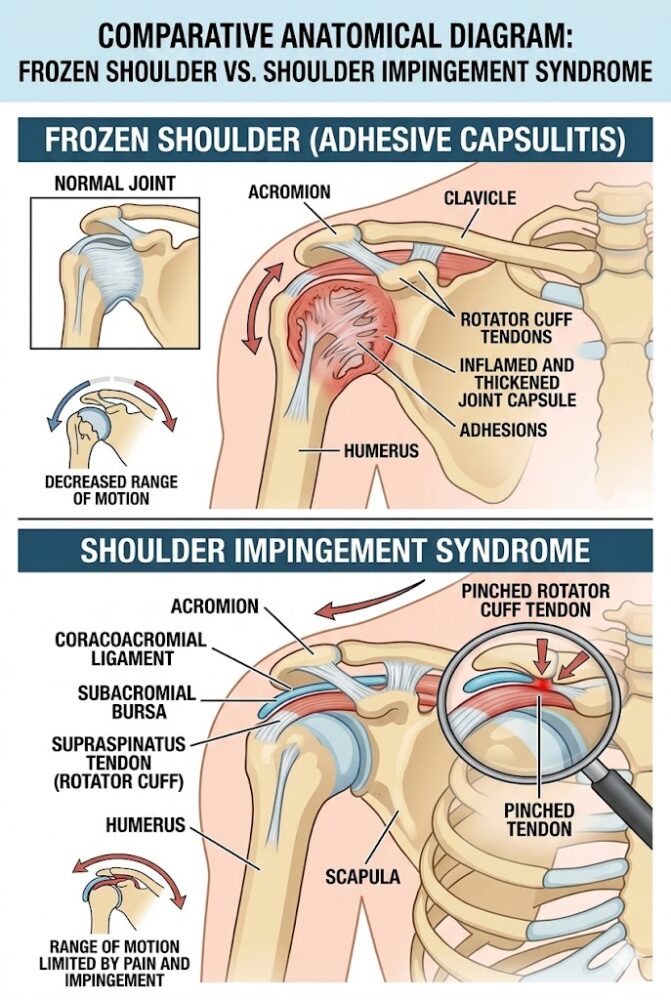
Consider these two familiar scenarios:
You went for an intense weekend badminton session in Puchong. Now, every time you attempt an overhead smash or reach back to grab a bag from your car’s back seat, a sharp, pinching pain stops you cold.
You wake at 2 a.m. with a deep, dull ache. Over the past few months, the joint has grown progressively stiffer. You can no longer reach your back pocket, wash your hair comfortably, or hook your bra.
If either scenario sounds familiar, read on. This clinical guide will help you identify your condition, understand the Malaysian-specific risk factors, and determine the fastest path to a full recovery.
What Is Frozen Shoulder (Adhesive Capsulitis)?
Frozen shoulder, clinically termed adhesive capsulitis, is a progressive condition in which the connective tissue capsule surrounding the shoulder joint becomes inflamed, thickens, and contracts — physically restricting movement in virtually all directions.
Key clinical characteristics:
- The Definitive Sign: Loss of range of motion is global. Even when a physiotherapist or doctor attempts to passively lift your relaxed arm for you, the movement is physically blocked — not just painful.
- Three Clinical Stages: The condition progresses through a freezing phase (worsening pain and stiffness), a frozen phase (maximum stiffness, pain may reduce), and a thawing phase (gradual mobility returns).
- Who Is at Risk: Most prevalent in adults aged 40 to 60, with a significantly higher incidence among women. According to the Ministry of Health Malaysia (MyHealth), there is a well-established clinical link to diabetes and thyroid disorders — conditions that are highly prevalent in the Malaysian population.
- Post-Immobility Trigger: The condition commonly develops following prolonged arm immobility after a fracture, surgery, or stroke.
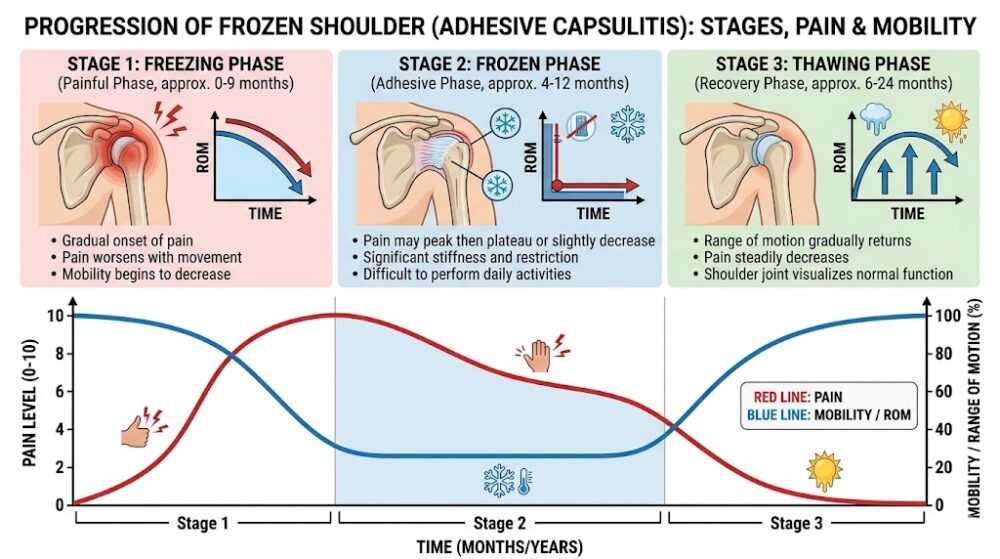 The three clinical stages of frozen shoulder: freezing, frozen, and thawing — each requiring a different physiotherapy approach.
The three clinical stages of frozen shoulder: freezing, frozen, and thawing — each requiring a different physiotherapy approach.What Is Shoulder Impingement Syndrome?
Shoulder impingement syndrome occurs when the rotator cuff tendons are repeatedly pinched or compressed against the underside of the acromion bone as they pass through the narrow subacromial space, causing pain at specific movement angles.
Key clinical characteristics:
- The Definitive Sign: Full passive range of motion is typically preserved, but a sharp, catching pain is triggered at a “painful arc” — classically when lifting the arm out to the side or overhead between 60 and 120 degrees.
- Who Is at Risk: Athletes performing repetitive overhead movements, and individuals with a forward-rounded shoulder posture from prolonged desk work.
- The Badminton Factor: Badminton’s repetitive high-velocity overhead smash directly drives the rotator cuff tendons into the acromion. It is not coincidental that Malaysia — a nation of badminton players — has an exceptionally high rate of sport-induced impingement.
- The Klang Valley Posture Factor: Extended periods spent stationary in traffic jams along the LDP, Sprint Highway, or Federal Highway — followed immediately by hours hunching over a laptop — creates a chronic forward-rounded shoulder posture (which is also a leading cause of cervicogenic headaches and neck pain). This postural pattern structurally narrows the subacromial space, making sedentary office workers nearly as vulnerable to tendon pinching as competitive athletes.
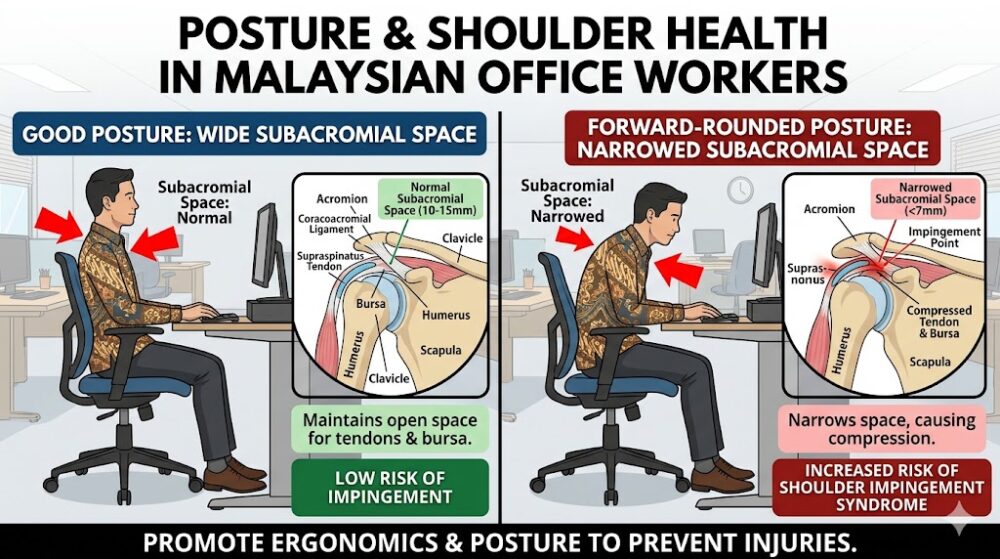 Forward-rounded posture from prolonged desk work or driving narrows the subacromial space — a key risk factor for shoulder impingement in Klang Valley office workers.
Forward-rounded posture from prolonged desk work or driving narrows the subacromial space — a key risk factor for shoulder impingement in Klang Valley office workers.Frozen Shoulder vs. Impingement: What Is the Key Difference?
The primary clinical distinction is this: a frozen shoulder physically prevents the arm from moving passively in all directions, whereas shoulder impingement allows a full range of passive movement but triggers sharp pain at specific overhead angles.
Use this quick self-assessment checklist before your clinical consultation:
| Assessment Test | Points to Frozen Shoulder | Points to Impingement |
|---|---|---|
| Passive Movement | A helper cannot raise your relaxed arm — it feels physically blocked | A helper can raise your arm fully, but it hurts at mid-range |
| Pain Character | Deep, dull, constant ache; relentless at night | Sharp, catching, or pinching sensation during specific movements |
| Pain Location | Diffuse throughout the entire joint | Localised to the outer shoulder or top of the arm |
| Onset Pattern | Gradual stiffening over weeks to months | Linked to specific activity (sport, overhead work, posture) |
| Night Pain | Severe — wakes patient from sleep; worse lying on affected side | Mild to moderate; usually not severe enough to wake patient |
| Affected Age Group | 40–60 years; higher risk with diabetes or thyroid disorder | Any age; higher risk in badminton players and desk workers |
Physiotherapy Treatment: What Works for Each Condition
Because the underlying pathology is fundamentally different, the physiotherapy approach for frozen shoulder and shoulder impingement must be entirely different — and using the wrong protocol will delay your recovery significantly.
Treating Frozen Shoulder (Adhesive Capsulitis)
- Pendulum exercises — gravity-assisted gentle mobilisation to preserve available range
- Passive joint mobilisation by a physiotherapist — carefully graded capsular stretching
- Heat therapy (moist heat packs) before exercise to increase capsular extensibility
- Corticosteroid injection (administered by a doctor) during the freezing phase to reduce inflammation
- Hydrodilatation — a procedure that stretches the contracted capsule using injected fluid
- Patience — the thawing phase can take 12–24 months without intervention; physiotherapy compresses this timeline
Treating Shoulder Impingement Syndrome
- Rotator cuff strengthening — targets the infraspinatus, supraspinatus, and teres minor to stabilise the humeral head
- Scapular stabilisation exercises — corrects the winging or elevation that narrows the subacromial space
- Postural retraining — corrects the forward-rounded shoulder posture that structurally compresses the tendons
- Dry needling to the infraspinatus and upper trapezius — highly effective for sport-related impingement
- Activity modification — temporary reduction of overhead loading (badminton, swimming breaststroke)
- Return-to-sport programming — structured progression back to badminton or overhead work with correct biomechanics
Red Flags: When to See a Doctor Immediately (Not Just a Physiotherapist)
Do not self-manage shoulder pain if any of the following are present:
- Sudden severe shoulder pain after a fall or collision — possible rotator cuff tear or fracture
- Shoulder pain accompanied by chest pain, shortness of breath, or left arm radiation — rule out cardiac origin immediately
- Visible deformity, swelling, or bruising after trauma
- Night sweats, unexplained weight loss, or fever alongside shoulder pain — possible systemic or neoplastic cause
- Complete inability to lift the arm at all, with no prior history of stiffness
Frequently Asked Questions About Shoulder Pain in Malaysia
The core difference is passive range of motion. In frozen shoulder (adhesive capsulitis), the shoulder joint capsule physically contracts, preventing movement in all directions — even when someone else tries to move your relaxed arm for you. In shoulder impingement syndrome, the joint can still move through a full range passively, but a sharp “painful arc” of pain occurs at specific overhead angles (typically 60–120 degrees) as the rotator cuff tendons are pinched under the acromion.
Without structured physiotherapy intervention, frozen shoulder can last 18 months to 3 years before naturally resolving. Even after natural resolution, many patients are left with a permanent reduction of 10–20 degrees of motion. With evidence-based physiotherapy — particularly graded joint mobilisation and capsular stretching — the thawing phase can be compressed to 6–12 months. Malaysian patients with comorbid diabetes or thyroid conditions are at risk of a longer and more severe course.
Yes — and it is the single most common sport-related cause of shoulder impingement in Malaysia. The overhead smash in badminton is a ballistic movement that drives the humeral head upward, repeatedly compressing the supraspinatus tendon against the underside of the acromion. Weekend warriors who play infrequently but at high intensity (the “weekender” pattern common in Klang Valley recreational leagues) are at particularly high risk, as their rotator cuff muscles are under-conditioned relative to the forces being generated.
Yes — significantly so. Clinical literature consistently reports that people with Type 2 diabetes are 3–5 times more likely to develop frozen shoulder than the general population. The mechanism is believed to involve advanced glycation end-products (AGEs) that cross-link collagen fibres in the joint capsule, causing it to thicken and contract. Given Malaysia’s high rate of Type 2 diabetes, this is a major risk factor for the local population. Diabetic patients with frozen shoulder also tend to experience a more severe, bilateral (both shoulders), and longer-lasting presentation.
Private physiotherapy in the Sungai Buloh, Petaling Jaya, and Klang Valley corridor typically costs RM 80 to RM 180 per session. A standard course of treatment for shoulder impingement (8–12 sessions) would typically total RM 800–RM 2,000. Frozen shoulder treatment, which requires more sessions over a longer course, may total RM 2,000–RM 4,000 for a full recovery programme. Patients with private medical insurance should verify whether their policy includes an outpatient physiotherapy benefit or a post-surgical rehabilitation rider.
See a physiotherapist first if your shoulder pain has a gradual onset, is activity-related, has been present for less than 3 months, and there is no history of trauma. A good physiotherapist will screen for red flags during your first assessment and refer you to an orthopaedic specialist or sports medicine physician if the presentation suggests a structural issue requiring imaging (MRI, ultrasound) or injection. If you have had a fall or collision, or suspect a rotator cuff tear, consult a doctor or specialist directly.
Yes — the vast majority of shoulder impingement cases resolve fully with conservative physiotherapy alone. Studies consistently show that 60–80% of patients with shoulder impingement achieve full functional recovery through a structured programme of rotator cuff strengthening, scapular stabilisation, and postural correction without surgical intervention. Surgery (subacromial decompression) is typically only considered after a minimum of 3–6 months of consistent physiotherapy has failed to produce improvement.
During the freezing phase (when pain is at its worst), avoid any aggressive stretching or forcing of movement — this can worsen the inflammatory response and accelerate capsular contraction. Specifically avoid: aggressive overhead reaching, behind-the-back stretches, pull-up or chin-up type movements, and heavy lifting. Gentle pendulum exercises and heat-assisted passive stretching within pain-free range are appropriate. In the frozen phase (when pain reduces but stiffness is maximal), more progressive physiotherapist-guided mobilisation is appropriate — but should always be performed under clinical supervision.
📅 Book Your Shoulder Pain Assessment in the Klang Valley
Whether you suspect frozen shoulder or impingement, the right diagnosis is everything. Our vetted physiotherapy partners across Sungai Buloh and the Klang Valley provide accurate clinical assessment and condition-specific rehabilitation from the very first session.
Or WhatsApp Your Nearest Location
📍 Local Note:
This article is produced by the ServicePro.my Healthcare Editorial Team for informational purposes only. It does not constitute medical advice. Always consult a licensed healthcare professional — including a registered physiotherapist, orthopaedic surgeon, or GP — for diagnosis and individualised treatment planning.



