Regaining Control: How Neurological Physiotherapy Manages Parkinson’s Symptoms in Sungai Buloh
For family caregivers in Sungai Buloh, Shah Alam, and the broader Klang Valley — an evidence-based guide to specialist neurological rehabilitation for Parkinson’s disease, beyond medication management.
Book Clinical Assessment Now
Who This Article Is For: Family caregivers in Sungai Buloh, Shah Alam, and the broader Klang Valley who are recognising early signs of neurological decline or managing an elderly parent’s Parkinson’s disease and are actively searching for evidence-based, specialist-led rehabilitation — not just medication management.
What Is Neurological Physiotherapy, and How Is It Different from Regular Physio for Parkinson’s Disease?
Neurological physiotherapy is a clinical specialisation focused exclusively on rehabilitating patients whose movement impairments originate in the central nervous system (CNS) — and for Parkinson’s disease, it is a gold-standard non-pharmacological intervention recommended by neurologists and advocacy groups like the Malaysian Parkinson's Disease Association (MPDA).
Standard physiotherapy after, say, a knee replacement, targets the musculoskeletal system — strengthening torn ligaments or rebuilding atrophied muscle tissue. Neurological physiotherapy operates at a fundamentally different level. It leverages the brain’s capacity for neuroplasticity — the ability to form new neural pathways and “reroute” motor signals around damaged circuits in the basal ganglia, the region of the brain most affected by Parkinson’s disease.
In practical terms, this means:
- Task-specific repetitive training to engrain compensatory movement patterns into procedural memory
- Sensory cue therapy (auditory, visual, and tactile cues) to bypass the defective internal rhythm-generation system of the Parkinson’s brain
- Gait re-education targeting the characteristic shuffling gait (festination), freezing of gait (FOG), and stooped posture
- Balance and proprioception retraining to directly address the elevated fall risk that makes Parkinson’s so dangerous for elderly Malaysians living in multi-storey terrace houses or condominiums with tiled floors
Key Distinction: A general physiotherapist will strengthen your parent’s quadriceps. A neurological physiotherapist will retrain how the brain commands the legs to move.
What Causes the “Shuffling Gait” in Parkinson’s Disease — and Can It Actually Be Improved?
The Parkinson’s shuffling gait is a direct neurological symptom, not a muscle weakness problem, and it can be functionally improved with targeted neurological rehabilitation.
The Neuroscience Behind the Shuffle
The shuffling gait — clinically termed festinating gait or hypokinetic gait — occurs because of the following cascade:
- Dopamine depletion in the substantia nigra disrupts the basal ganglia’s ability to generate automatic, rhythmic motor sequences — the “background programme” that normally runs walking without conscious effort.
- Loss of stride amplitude results as the basal ganglia can no longer scale movement size appropriately — each step becomes progressively shorter and lower-clearance, producing the characteristic small, shuffling steps.
- Festination develops as the brain attempts to compensate for loss of balance by accelerating step frequency — the patient takes faster and faster small steps to “catch up” with their own centre of gravity.
- Freezing of Gait (FOG) occurs when the defective internal rhythm generator stalls completely — typically at doorways, turns, or when attention is divided — causing the feet to feel “glued” to the floor.
- Postural instability compounds the problem as reduced trunk rotation, forward flexion, and a high-centre-of-gravity posture increase fall risk with every step taken.
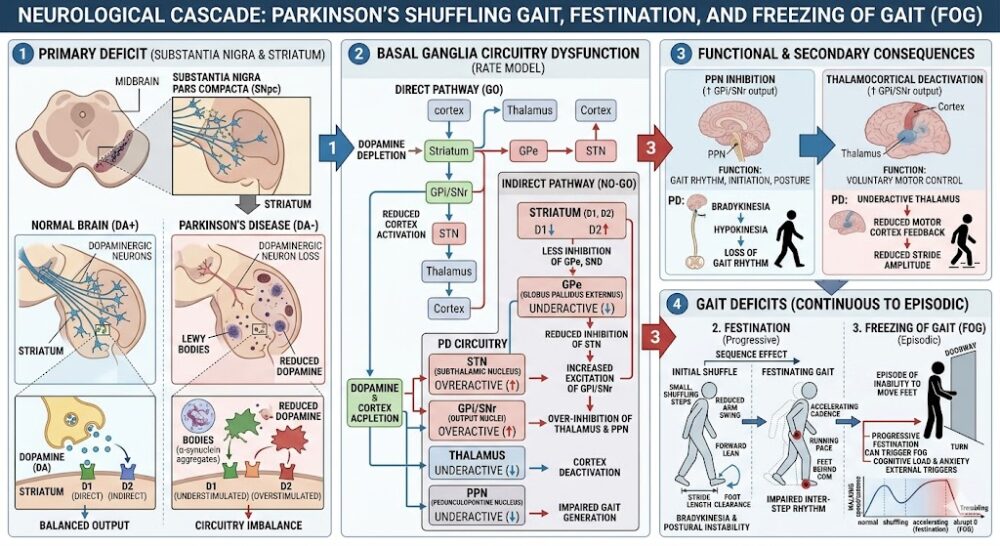 The neurological cascade from dopamine depletion to festinating gait — and why targeted neurological physiotherapy can interrupt this cycle at multiple points.
The neurological cascade from dopamine depletion to festinating gait — and why targeted neurological physiotherapy can interrupt this cycle at multiple points.Can it be improved? Yes — and this is precisely where neurological physiotherapy delivers measurable, evidence-backed results. Because the deficit lies in the automatic motor control system, physiotherapy applies external sensory cues (a metronome beat, rhythmic music, or floor markers) to shift gait control from the broken automatic system to the voluntary, conscious motor pathway — which is largely preserved in Parkinson’s disease. Clinical studies consistently demonstrate a 20–30% improvement in stride length and a significant reduction in FOG episodes with structured gait cue therapy.
The Six Parkinson’s Symptoms Neurological Physiotherapy Directly Targets
A specialist neurological physiotherapist does not treat Parkinson’s generically — they build a targeted programme around the specific movement impairments that are reducing your parent’s quality of life and increasing their fall risk.
Shuffling Gait & Festination
Auditory and visual cueing strategies to restore stride length and rhythm, reducing the risk of forward falls from accelerating, uncontrolled steps.
Freezing of Gait (FOG)
Attentional strategies and cueing techniques to allow the patient to bypass frozen episodes and initiate movement safely at doorways, turns, and in crowds.
Balance Impairment & Falls
Targeted postural stability exercises and reactive balance training to reduce the fall incidence that is the leading cause of hospitalisation in Parkinson’s patients.
Bradykinesia (Slowness of Movement)
High-amplitude, large-movement exercises (LSVT BIG protocol) to recalibrate the brain’s perception of movement size and restore normal speed and amplitude to daily activities.
Stooped Posture (Camptocormia)
Spinal extension, core activation, and postural awareness training to counteract the progressive forward flexion posture that compresses the chest and disrupts balance.
Functional Independence in ADLs
Task-specific training for Activities of Daily Living (ADLs) — getting up from a chair, turning in bed, climbing stairs in a Malaysian terrace house — to maintain independence for as long as possible.
General Physio vs. Neurological Physio for Parkinson’s: What Is the Key Difference?
The fundamental difference lies in the target: general physiotherapy addresses muscle and joint impairment, while neurological physiotherapy targets the brain’s motor control system itself. Using the wrong approach will limit your parent’s recovery significantly.
| Clinical Factor | General Physiotherapy | Neurological Physiotherapy |
|---|---|---|
| Primary Target | Muscles, joints, and soft tissue | Central nervous system — neural pathways and motor control circuits |
| Gait Treatment | Strengthening leg muscles and improving range of motion | Sensory cueing (auditory, visual) to retrain stride length and rhythm at a neurological level |
| Balance Training | General proprioception and stability exercises | Reactive balance training with perturbation therapy, targeting the Parkinson’s-specific postural righting reflex deficit |
| Freezing of Gait | Not specifically addressed | FOG-specific cueing strategies, attentional focus techniques, and dual-task training |
| Bradykinesia | Not specifically addressed | LSVT BIG protocol — high-amplitude movement recalibration to restore normal movement size |
| Outcome Goal | Reduce pain; restore post-injury function | Slow disease progression impact; preserve independence; reduce fall risk over the long term |
Physiotherapy Treatment: What a Parkinson’s Neurological Rehab Programme Includes
A specialist neurological physiotherapy programme for Parkinson’s disease is structured across two parallel tracks: motor rehabilitation to address movement impairments, and fall prevention to protect your parent’s safety and independence.
Motor Rehabilitation Programme
- LSVT BIG training — high-amplitude, large-scale movement exercises to recalibrate the brain’s movement-size perception
- Auditory rhythmic cueing (ARC) — metronome-based gait training to restore stride length and walking cadence
- Visual floor cue training — floor markers and tape lines to guide step length and navigate doorways without freezing
- Postural correction exercises — targeted spinal extension and core activation to counteract camptocormia (stooped posture)
- Trunk rotation and reciprocal arm swing — restoring the counter-rotation movement that is lost early in Parkinson’s disease
- Transfer training — safely getting up from chairs, beds, and the floor — critical for Malaysian homes with low seating
Balance & Fall Prevention Programme
- Reactive postural training — supervised perturbation exercises to retrain the righting reflexes impaired by Parkinson’s
- Dual-task training — practising movement while performing a cognitive task, simulating the real-world conditions that most commonly trigger falls
- Stair and ramp negotiation — specific training for Malaysian terrace house staircases and wet bathroom floor surfaces
- Home environment assessment — identifying and modifying fall hazards in the patient’s specific living environment
- Assistive device training — correct use of walking aids and rollator walkers to prevent the compensatory stumbling that increases fall risk
- Caregiver education — guiding family members on how to safely assist during freezing episodes and transfers
When to See a Neurologist or Specialist Doctor First (Not Just a Physiotherapist)
Seek urgent medical review — not self-managed physiotherapy — if your parent experiences any of the following:
- A sudden, marked worsening of symptoms over days — possible medication interaction, infection, or Parkinson’s crisis (akinetic crisis)
- Sudden severe confusion, hallucinations, or aggressive behaviour alongside motor changes — possible Parkinson’s dementia complication or medication side effect
- A fall with head impact, loss of consciousness, or inability to bear weight — immediate A&E attendance required
- Rapid unintended weight loss, difficulty swallowing (dysphagia), or choking — possible advanced disease progression requiring specialist review
- New asymmetric weakness, facial droop, or speech changes — must rule out concurrent stroke, which presents differently to Parkinson’s
📍 Local Note: This guide is written for patients and caregivers in Sungai Buloh and the Klang Valley corridor. Neurology departments and specialist centres nearby include Hospital Sungai Buloh (HSB), Hospital Kuala Lumpur (HKL) — Neurology Department, Subang Jaya Medical Centre (SJMC), and KPJ Damansara Specialist Hospital. For post-diagnosis neurological physiotherapy, our vetted rehabilitation partners serve patients across Sungai Buloh, Kepong, Shah Alam, Petaling Jaya, Damansara, and surrounding areas.
Frequently Asked Questions About Parkinson’s Physiotherapy in Malaysia
Neurological physiotherapy is a clinical specialisation that targets the central nervous system — not just muscles and joints. For Parkinson’s, a neurological physiotherapist uses techniques like sensory cueing, LSVT BIG training, and reactive balance perturbation to retrain the brain’s motor control circuits. General physiotherapy addresses musculoskeletal problems such as a torn ligament or weak quadriceps — it does not address the basal ganglia dysfunction that causes the shuffling gait, freezing episodes, and postural instability of Parkinson’s disease.
Physiotherapy does not slow the neurochemical progression of Parkinson’s disease — it cannot replace dopamine or halt the degeneration of the substantia nigra. What it demonstrably does is slow the functional decline that results from the disease. By maintaining gait quality, balance, trunk mobility, and muscle strength, consistent neurological physiotherapy preserves independence and reduces fall risk for significantly longer than medication management alone. Clinical evidence consistently shows that exercise and structured rehabilitation are the most powerful non-pharmacological interventions available for Parkinson’s patients.
Your neurological physiotherapist will teach you specific strategies during your parent’s sessions. The most effective home techniques include: counting out loud (“1, 2, 3, go”) to engage the voluntary motor pathway; shifting weight from side to side before attempting to step; using a visual cue — place a strip of tape on the floor in front of doorways and tell your parent to “step over the line”; and marching on the spot to re-initiate gait rhythm. Importantly, do not pull your parent’s arm to force movement during a freeze — this increases fall risk significantly. Freeze episodes typically last 5–30 seconds; remaining calm and applying one cue at a time is the safest approach.
Yes — and timing your parent’s physiotherapy sessions relative to their medication “on” window is clinically important. Levodopa (carbidopa-levodopa, sold as Madopar or Sinemet in Malaysia) typically produces a motor “on” period 30–60 minutes after ingestion. Scheduling physiotherapy sessions during this window — when the patient’s motor function is at its daily peak — significantly improves the quality and intensity of gait and balance training. Your neurological physiotherapist will coordinate with your parent’s neurologist regarding optimal session timing. Exercise does not interfere with levodopa absorption and is considered safe and highly recommended alongside pharmacological management.
Unlike injury rehabilitation with a defined endpoint, Parkinson’s physiotherapy is an ongoing, lifelong programme that adapts as the disease progresses. A typical initial intensive block is 2–3 sessions per week for 6–8 weeks, followed by a maintenance programme of 1–2 sessions per week indefinitely. Private neurological physiotherapy in the Sungai Buloh and Klang Valley corridor typically costs RM 100 to RM 200 per session, depending on session duration and the specific protocols used. Patients with private medical insurance should verify whether their policy includes an outpatient neurological rehabilitation benefit. Long-term, the cost of consistent physiotherapy is significantly lower than the direct and indirect cost of a single fall-related hospitalisation.
Yes, and your physiotherapist must be informed of both conditions. Diabetic peripheral neuropathy — which is highly prevalent among Malaysian Type 2 diabetics — compounds the balance and proprioception deficits of Parkinson’s, creating a significantly elevated fall risk profile. A neurological physiotherapist will modify the balance training protocol to account for reduced sensory feedback from the feet, increase the use of visual compensation strategies, and monitor for hypoglycaemia during exercise sessions. Blood glucose levels should be checked before each session, and the physiotherapist should be aware of your parent’s medication schedule. This combined presentation is common in the Malaysian elderly population and experienced neurological physiotherapists in the Klang Valley regularly manage it.
As early as possible after diagnosis — ideally at Hoehn & Yahr Stage 1 or 2, before significant functional decline has occurred. The neuroplastic capacity of the brain is greatest in the earlier stages, meaning that gait patterns, balance reflexes, and movement amplitude can be most effectively retrained before they have substantially deteriorated. Many caregivers in Malaysia wait until their parent experiences a serious fall or becomes unable to manage stairs before seeking physiotherapy — at which point rehabilitation is more difficult and the intervention window is narrower. Starting early does not mean committing to daily intensive sessions; even a monthly review with a home exercise programme can significantly slow the functional decline trajectory in early-stage Parkinson’s.
Not all physiotherapists have specialist neurological training or clinical experience with Parkinson’s disease. When evaluating a physiotherapy centre, ask specifically whether the physiotherapist has experience with Parkinson’s disease rehabilitation, whether they are familiar with LSVT BIG, auditory rhythmic cueing, and FOG management protocols, and whether they conduct a standardised Parkinson’s-specific outcome assessment (such as the Berg Balance Scale, Timed Up and Go, or the Unified Parkinson’s Disease Rating Scale motor subscale). Our vetted physiotherapy partners in Sungai Buloh and the Klang Valley have been selected specifically for their neurological rehabilitation expertise — tap your location below to be connected directly via WhatsApp.
📅 Book Your Parkinson’s Neurological Physiotherapy Assessment in the Klang Valley
Whether your parent is newly diagnosed or managing advanced Parkinson’s symptoms, the right neurological physiotherapy programme makes a measurable difference. Our vetted specialist partners across Sungai Buloh and the Klang Valley provide condition-specific Parkinson’s rehabilitation from the very first session.
The information in this article is intended for general educational purposes and does not constitute medical advice. Always consult a clinician registered with the Malaysian Medical Council (MMC) or a physiotherapist registered with the Malaysian Physiotherapy Association (MPA) for a diagnosis and personalised treatment plan. ServicePro.my connects Malaysians with vetted, verified healthcare and home service professionals across the Klang Valley and beyond.