Slipped Disc Treatment in Klang Valley: Physiotherapy vs. Surgery for Sciatica
For urban professionals enduring long KL commutes and desk-bound workdays, lumbar spine injuries have quietly become one of the most common musculoskeletal complaints seen in Klang Valley private clinics. This guide gives you the clinically grounded breakdown of both treatment pathways.
What Is a Slipped Disc, and Why Does It Cause Sciatica?
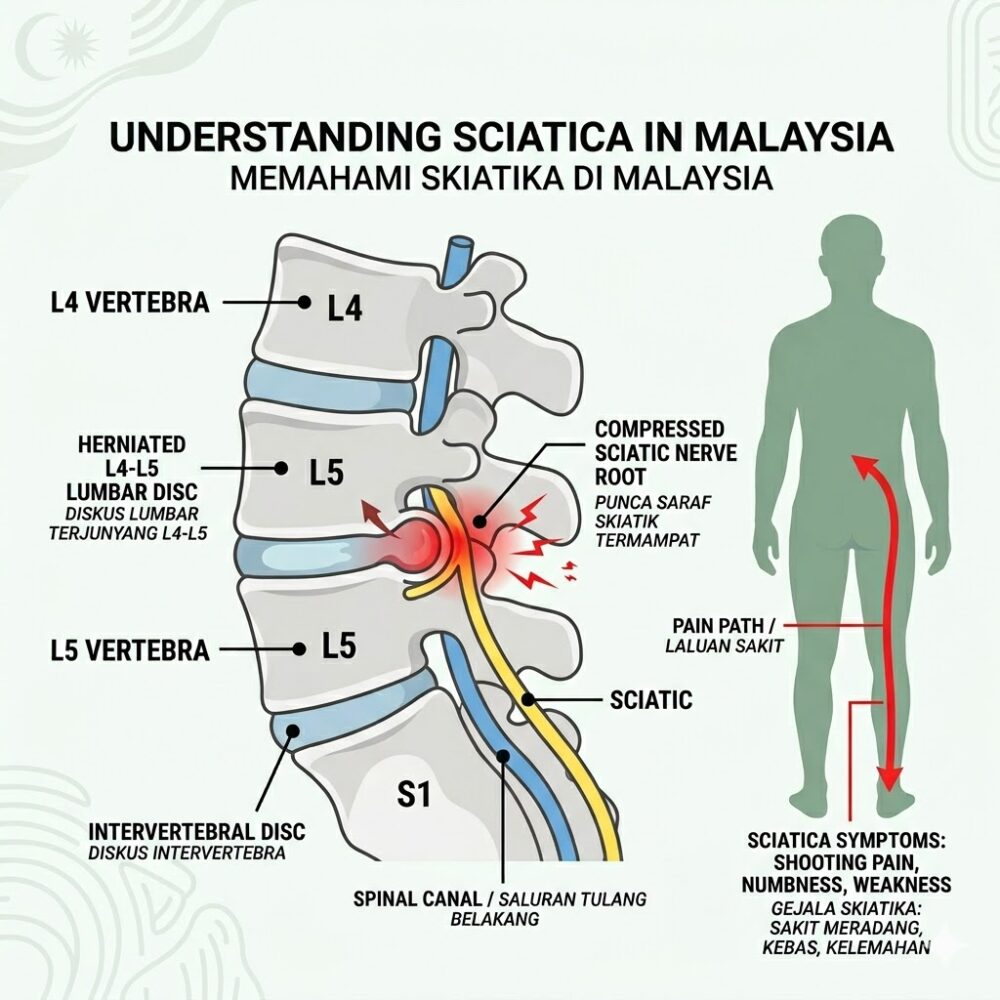
A slipped disc — clinically termed a lumbar disc herniation — occurs when the nucleus pulposus (the soft, gel-like interior of an intervertebral disc) breaches the annulus fibrosus (its tough outer casing) and protrudes into the spinal canal, directly compressing adjacent nerve roots.
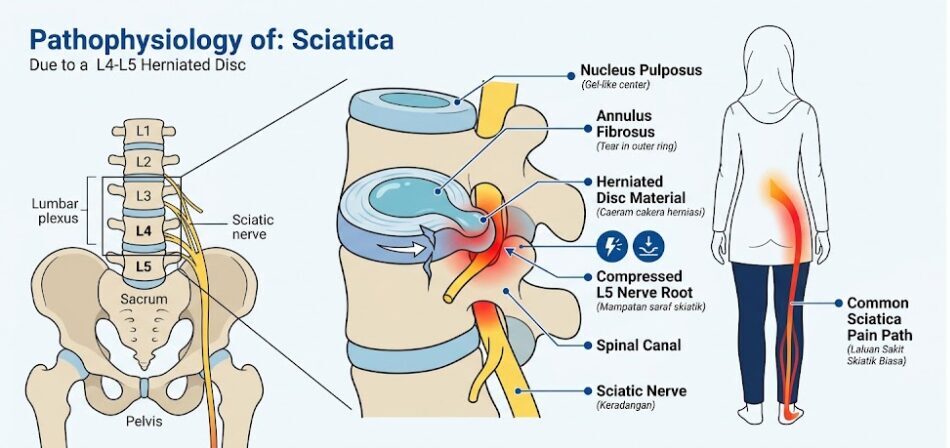
This mechanical compression, combined with the pro-inflammatory cytokines released by the exposed disc material, directly irritates the sciatic nerve — the body's longest peripheral nerve, running from the lumbar spine through the buttocks and down to the toes. The result is sciatica: a constellation of symptoms that should not be confused with ordinary lower back pain.
Classic Sciatica Symptoms Include:
Radiating Leg Pain
An electric shock or burning sensation that travels from the lower back, through the buttock, and down the posterior thigh into the calf or foot — typically affecting one side.
Dermatomal Numbness
"Pins and needles" or complete sensory loss in a specific strip of skin correlating to the compressed nerve root (commonly L4, L5, or S1).
Motor Weakness
Difficulty dorsiflexing the foot (foot drop), standing on tiptoes, or bearing weight on the affected limb.
Positional Aggravation
Sharp pain spikes during coughing, sneezing, or prolonged sitting — a daily reality for patients stuck in PJ–KL morning traffic.
Clinical Note: Not all lower back pain is a slipped disc, and not all disc herniations cause sciatica. An accurate diagnosis from a registered physiotherapist or orthopaedic specialist is essential before any treatment protocol begins.
How Is a Slipped Disc Diagnosed in Malaysia?
Slipped disc diagnosis in Malaysia combines clinical neurological testing with imaging, and an MRI scan of the lumbar spine remains the gold-standard investigation. A trained physiotherapist or orthopaedic surgeon will typically follow this diagnostic pathway:

Clinical Assessment
Before any imaging is ordered, clinicians use specific provocative tests to identify nerve root involvement:
Straight Leg Raise (SLR) Test
Lifting the patient's straightened leg to 30–70° reproduces sciatic pain, indicating nerve root irritation.
Slump Test
A seated neural tension test that reproduces leg symptoms, confirming sciatic nerve involvement.
Dermatomal Mapping
Assessing sensory deficits across the leg to identify which nerve root level (L3, L4, L5, or S1) is compressed.
Myotomal Testing
Checking muscle strength at specific levels (e.g., big toe extension for L5, ankle plantarflexion for S1).
Imaging Investigations
| Investigation | Purpose | Estimated Cost in Malaysia |
|---|---|---|
| MRI Lumbar Spine | Definitive disc herniation confirmation; shows nerve compression | RM 800 – RM 1,500 |
| X-Ray (AP & Lateral) | Rules out fractures and spondylolisthesis; does not visualise soft tissue | RM 80 – RM 200 |
| CT Scan | Used when MRI is contraindicated (e.g., pacemaker patients) | RM 500 – RM 1,000 |
| Nerve Conduction Study (NCS/EMG) | Quantifies motor nerve damage; informs surgical planning | RM 400 – RM 800 |
Important: An MRI is not mandatory before beginning physiotherapy. If symptoms are consistent with a clinical diagnosis and no red flags are present, a registered physiotherapist may begin conservative treatment immediately and request imaging only if symptoms fail to progress.
What Does Physiotherapy for a Slipped Disc Actually Involve?
A structured physiotherapy programme for lumbar disc herniation addresses nerve decompression, pain modulation, and spinal stability simultaneously — not just symptom relief.

An evidence-based programme delivered by a registered physiotherapist (registered with the Malaysian Physiotherapy Association, MPA) will typically progress through three structured phases:
Acute Pain Management
The priority in this phase is reducing neural inflammation, restoring basic mobility, and eliminating protective muscle spasm.
- Manual Therapy: Joint mobilization and soft tissue release techniques to reduce acute lumbar muscle guarding
- Modalities: Therapeutic ultrasound, interferential therapy (IFT), or TENS to modulate pain signals
- Neural Mobilisation: Gentle nerve flossing and sciatic nerve glides to reduce adhesion around the nerve root
- Postural Education: Correct sitting, standing, and sleep posture to minimise compressive load on the herniated segment
Functional Recovery
Once acute pain is controlled, rehabilitation shifts to motor retraining and spinal reconditioning.
- McKenzie Method (MDT): Directional preference exercises specifically designed to centralise pain — moving symptoms from the foot back toward the spine
- Spinal Decompression Therapy: Mechanical or manual traction applied to the lumbar spine to create negative intradiscal pressure, encouraging the herniated nucleus to retract
- Core Stabilisation Programme: Systematic activation and strengthening of the transverse abdominis, multifidus, and pelvic floor
Maintenance and Relapse Prevention
Long-term spinal health and relapse prevention through lifestyle integration.
- Ergonomic Assessment: Particularly relevant for KL and PJ-based desk workers; posture correction for prolonged sitting, laptop positioning, and car seat ergonomics
- Progressive Loading: Return to sport, gym, or demanding physical work through graded exposure
- Home Exercise Programme: A personalised, independent routine to sustain spinal health long-term
For a comprehensive, supervised rehabilitation programme, residents across Selangor and the Klang Valley can book an initial assessment at a verified slipped disc physiotherapy centre in Sungai Buloh, where certified physiotherapists conduct thorough neurological assessments and build individualized recovery roadmaps.
When Is Spinal Surgery Actually Necessary? Recognising the Red Flags
Spinal surgery for a slipped disc is medically necessary in a minority of cases — but when these clinical red flags are present, delay can result in permanent neurological damage.
Orthopaedic surgeons and neurosurgeons in Malaysia will recommend proceeding directly to surgical intervention — bypassing the physiotherapy trial — if any of the following are present:
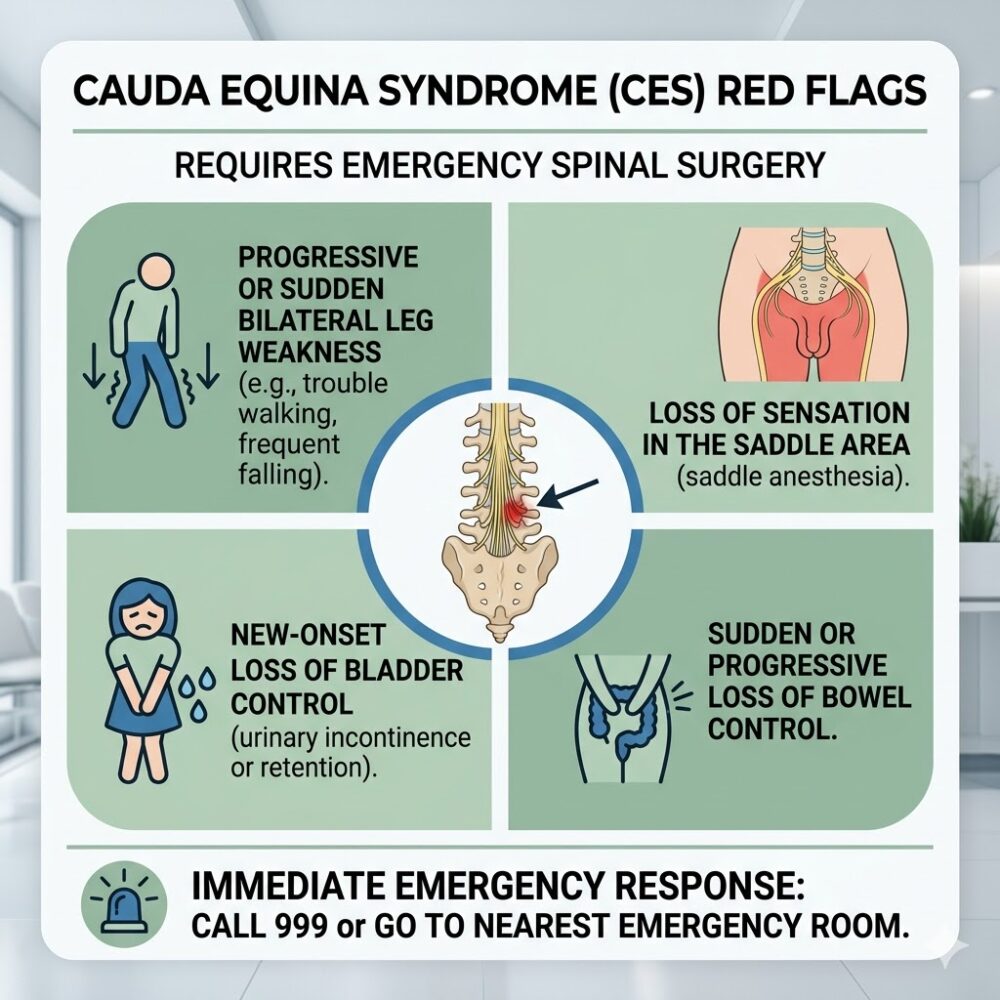
Absolute Surgical Emergencies — Seek A&E Immediately
- Cauda Equina Syndrome (CES): Compression of the terminal spinal nerve bundle causing bilateral leg weakness, saddle anaesthesia (numbness in the groin and inner thighs), and — critically — loss of bowel or bladder control. This is a neurosurgical emergency; irreversible damage can occur within hours if not decompressed.
- Rapidly Progressive Motor Deficit: Sudden or rapidly worsening foot drop, inability to lift the leg, or bilateral lower limb weakness indicating acute severe nerve compression.
Relative Surgical Indications — Discuss with Specialist
- Intractable, unremitting pain: Debilitating sciatica that fails to respond to a minimum of 6–8 consecutive weeks of intensive, supervised physiotherapy and appropriate pharmacological management (NSAIDs, neuropathic pain agents, epidural steroid injections).
- Confirmed large disc herniation with significant neural compromise: MRI evidence of a sequestrated or extruded fragment causing severe canal stenosis, paired with worsening clinical findings.